
Hormone Therapy
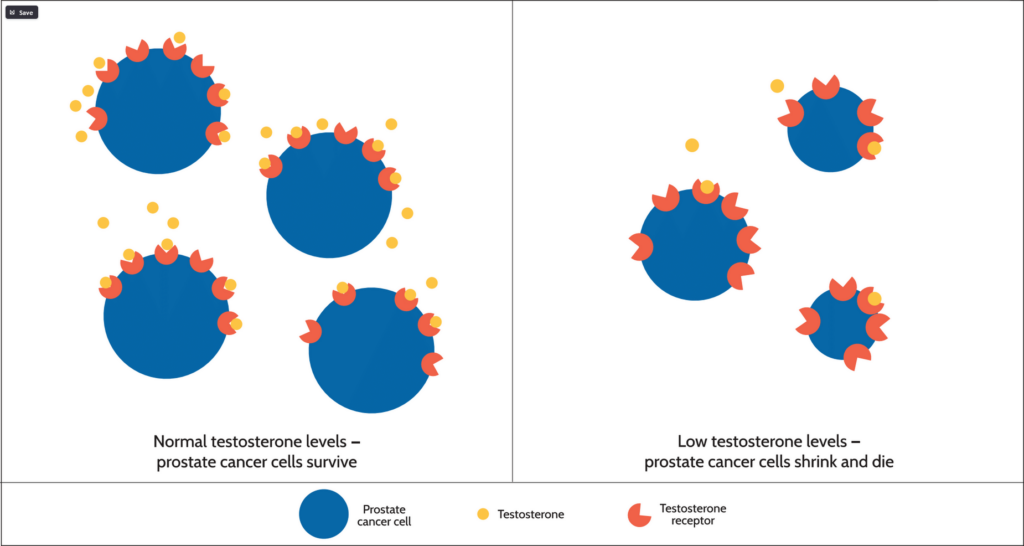
Hormone therapy is designed to inhibit testosterone production or directly block it from acting on prostate cancer cells. It is, essentially, “anti-testosterone therapy.” The majority of prostate cancer cells will stop growing following the removal of testosterone, and many will die.
How Hormone Therapy Affects Prostate Cancer Cells
There are different forms of hormone therapy that work in different ways in your body. Most are given as regular injections, sometimes in combinations. These forms of hormone therapy have been used for decades. There are also newer androgen receptor pathway inhibitors for patients with certain types of advanced prostate cancer.
Surgery to remove the testicles (called orchiectomy) is another option. About 90% of testosterone is produced by the testicles. The procedure is typically done in the operating room as an outpatient procedure, with the majority of patients being discharged from the hospital on the same day. This is an option for men who prefer a low-cost, one-time procedure. Because it is irreversible, most patients opt for medical therapy.
The chart below lists different types of hormone therapy.
| Standard hormone therapy | Lower testosterone levels • Orchiectomy • LHRH agonists, e.g., leuprolide (Lupron, Eligard) • LHRH antagonists, degarelix (Firmagon), relugolix (Orgovyx) |
| Anti-androgens | Help block the action of testosterone Include: • Bicalutamide (Casodex) • Flutamide (Eulexin) • Nilutamide (Nilandron) |
| Androgen receptor pathway inhibitors | Newer medications approved for men with certain states of advanced prostate cancer • Abiraterone (Zytiga, Yonsa) • Apalutamide (Erleada) • Darolutamide (Nubeqa) • Enzalutamide (Xtandi) |
| LHRH Agonists | These medications work by acting on the release of LHRH, one of the key hormones that initiates the production of testosterone. They are given as regular shots: once a month, once every 3, 4, or 6 months, or once per year. LHRH agonists cause a “testosterone flare” reaction, which is an initial, temporary rise in testosterone and can cause a variety of symptoms. It can be prevented by co-treatment with anti-androgens. |
| LHRH Antagonists | These medications block LHRH from stimulating testosterone production without causing an initial testosterone surge. Relugolix is a newer, oral form with a faster mechanism of action. |
| Anti-Androgens | These drugs can help block the action of testosterone in prostate cancer cells. They are often given concurrently with some hormone injections to prevent symptoms/side effects of a testosterone flare. |
| Androgen Receptor Pathway Inhibitors | Also referred to as androgen receptor signaling inhibitors (ARSIs) or androgen receptor axis targeted agents (ARATs). Abiraterone blocks the production of testosterone, while apalutamide, darolutamide, and enzalutamide block the action of testosterone. These newer “second-generation” hormone treatments are FDA-approved for patients with certain states of advanced prostate cancer: high-risk biochemical recurrence (non-metastatic HSPC), mHSPC, non-metastatic castration-resistant prostate cancer (nmCRPC), and mCRPC. All are taken orally. Some are approved to be given in combination with other medicines. |
Last Reviewed: 12/2023


